Key takeaways
- ●"Peptides for longevity" is a search category, not a pharmacological mechanism — four distinct research categories intersect the longevity conversation.
- ●GH-axis (Mod GRF 1-29 + Ipamorelin) is the load-bearing category with the deepest research base in longevity-adjacent peptide work.
- ●The Peptide Lab carries six compounds across four categories and is transparent about what is excluded and why.
- ●No published controlled clinical lifespan data exists for any peptide compound — healthspan signal is preliminary.
- ●Multi-category stacking requires experimental designs that can distinguish individual contributions.
The framing: longevity is not a mechanism
“Peptides for longevity” is one of the highest-volume searches in the research-peptide space. The honest answer to the question is that no single peptide is a longevity compound — the category exists because several different research peptides intersect with biological systems that decline with age.
This guide maps those categories, names what each one actually addresses, and is transparent about what is and is not in scope on this site.
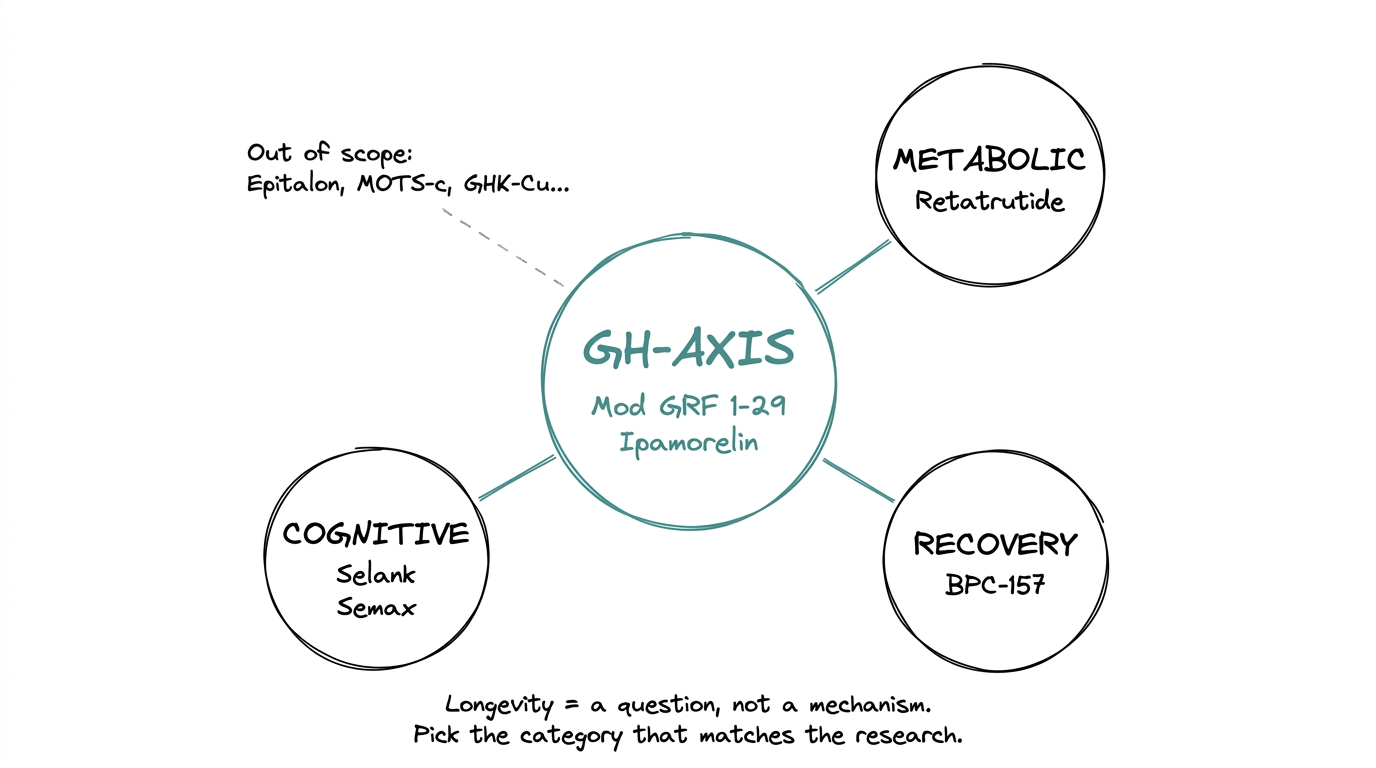
“Longevity” is a goal, not a pharmacological category. Different research peptides act on different biological systems that change with age. Grouping them under one heading is useful for navigation but misleading if it suggests they share a mechanism.
The cleaner mental model: pick the aging-related system you are interested in — growth hormone decline, metabolic dysregulation, tissue repair capacity, cognitive maintenance — and look at the compounds that are actually researched in that system.
1. GH-axis (the load-bearing category)
This is the most-researched longevity-adjacent category in the research-peptide space. The premise is simple: growth hormone secretion declines with age, and the question of whether restoring younger GH pulse patterns produces measurable downstream effects is one of the longest-running research programs in peptide pharmacology.
The two compounds that anchor this category in research-peptide work:
- ●Mod GRF 1-29 (also called CJC-1295 no DAC). A modified GHRH fragment that activates the GHRH receptor on pituitary somatotrophs.
- ●Ipamorelin. A selective ghrelin-receptor agonist that activates the GHS-R pathway without the cortisol and prolactin confound that earlier GH secretagogues produced.
The two are typically researched together as a stack because their pathways converge synergistically on the same somatotroph. The CJC-1295 + Ipamorelin guide covers the dual-pathway mechanism in detail.
What it addresses
Age-related GH pulse-amplitude decline, body-composition changes downstream of GH, sleep architecture and the nocturnal GH peak, IGF-1 dynamics.
What it does not address
Any direct cellular-aging mechanism (telomere length, mitochondrial dysfunction, senescent-cell clearance). GH-axis work is upstream-hormonal, not cellular-rejuvenation.
2. Metabolic (the GLP-1 / triple-agonist arm)
Metabolic dysregulation — insulin resistance, visceral adiposity, fatty liver — is one of the strongest correlates of accelerated biological aging. The metabolic-peptide category does not target aging directly, but it addresses a system that is downstream of aging and upstream of many age-related disease risks.
The compound that defines this category in current research:
- ●Retatrutide. A triple agonist activating GLP-1, GIP, and glucagon receptors, currently in Phase 3.
The earlier GLP-1 generation (semaglutide, tirzepatide) sits in the same category. Semaglutide is the FDA-approved reference. Retatrutide is the investigational frontier. The retatrutide vs Ozempic comparison covers the benchmark difference.
What it addresses
Body composition through energy intake and energy expenditure, glycemic control, hepatic fat oxidation, downstream metabolic-syndrome risk markers.
What it does not address
Any direct hormonal-axis or cellular-aging mechanism beyond the metabolic system itself.
3. Recovery (tissue-repair capacity as resilience)
Tissue repair capacity declines with age — tendons heal slower, mucosal integrity weakens, microinjury accumulates. This category is not framed as a longevity intervention, but it intersects the longevity conversation through the resilience angle: a research subject that recovers faster from microinjury accumulates less long-term damage.
The compound that anchors this category:
- ●BPC-157. A 15-amino-acid fragment of body protection compound that drives angiogenesis and cell-migration signaling through the FAK-paxillin pathway.
The BPC-157 vs TB-500 comparison covers the second compound that often shows up in this conversation, including why the two are mechanistically distinct rather than interchangeable.
What it addresses
Tendon and ligament repair, gastrointestinal mucosal integrity, microvascular regeneration in damaged tissue.
What it does not address
Primary aging mechanisms. Repair-capacity work is downstream-functional, not upstream-causal.
4. Cognitive (neurotransmitter modulation)
Cognitive decline is the most-feared part of aging in survey data, and the research-peptide space has two compounds that show up regularly in this conversation.
- ●Selank. A synthetic analogue of the tuftsin tetrapeptide. Researched for anxiolytic and cognitive-modulation effects through GABA, serotonin, and BDNF pathways.
- ●Semax. A synthetic ACTH(4-10) analogue. Researched for neuroprotective and cognitive-enhancement effects through BDNF and dopaminergic pathways.
Both are originally Russian compounds with most published research in Russian-language journals. Western preclinical replication is limited but growing.
What it addresses
Acute cognitive performance, anxiolysis, BDNF-pathway modulation, neuroprotection in stress and ischemia models.
What it does not address
Alzheimer's-disease-specific mechanisms (amyloid, tau), cellular neuroaging, or neurogenesis at scale.
How the categories relate to aging mechanisms
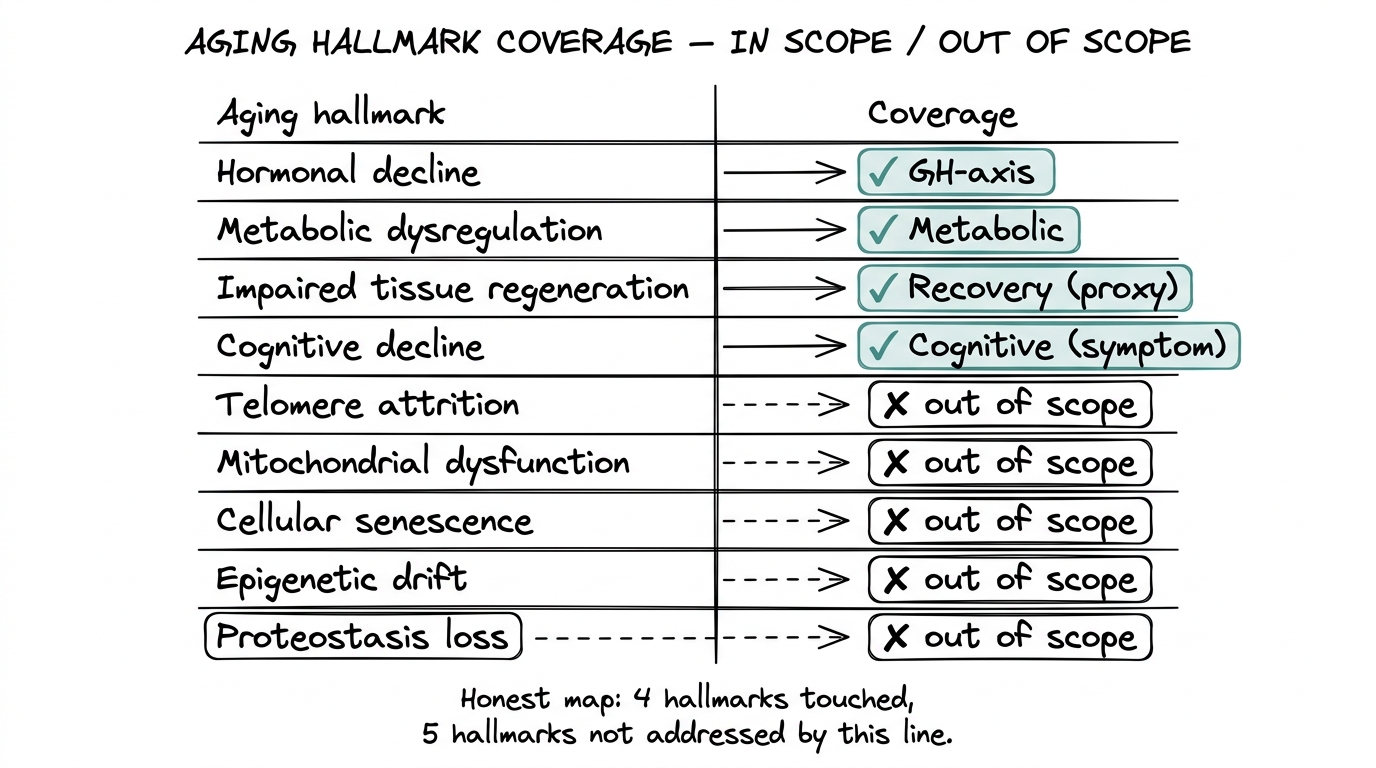
The honest mapping between aging mechanisms and research-peptide categories is uneven. Some hallmarks of aging have well-researched peptide counterparts; others have none in the current commercial research-peptide space.
| Aging hallmark | Peptide category | Coverage |
|---|---|---|
| Hormonal decline | GH-axis | Direct intersection |
| Metabolic dysregulation | Metabolic peptides | Direct intersection |
| Impaired tissue regeneration | Recovery peptides | Indirect (repair-capacity proxy) |
| Cognitive decline | Cognitive peptides | Indirect (symptom-axis modulation) |
| Telomere attrition | None in scope | Not addressed |
| Mitochondrial dysfunction | None in scope | Not addressed |
| Cellular senescence | None in scope | Not addressed |
| Epigenetic drift | None in scope | Not addressed |
| Proteostasis loss | None in scope | Not addressed |
Research peptides marketed as targeting the uncovered mechanisms (Epitalon for telomerase, MOTS-c for mitochondrial function, GHK-Cu for general “anti-aging”) exist in the broader supplement space but are not in scope here. The Peptide Lab carries the four categories above with research-grade documentation, not the broader anti-aging-claim category.
What the line includes vs what it does not
The transparent version: The Peptide Lab carries six research compounds across the four categories above.
In the line
GH-axis: Mod GRF 1-29 (CJC-1295 no DAC), Ipamorelin
Metabolic: Retatrutide
Recovery: BPC-157
Cognitive: Selank, Semax
Not in the line
Epitalon (telomere/pineal), MOTS-c (mitochondrial), GHK-Cu (copper peptide), Thymalin (immune-aging), NAD+ peptide variants, Sermorelin (different GHRH analogue), Tesamorelin (FDA-approved for HIV-associated lipodystrophy), and various longer GHRH analogues.
The omission is deliberate. Compounds with thinner published research, marketing-driven “anti-aging” framing, or unclear regulatory positioning sit outside the line. The category map above is honest about what is in and what is not.
How to choose between categories
The category-by-question framing is more useful than ranking compounds against each other.
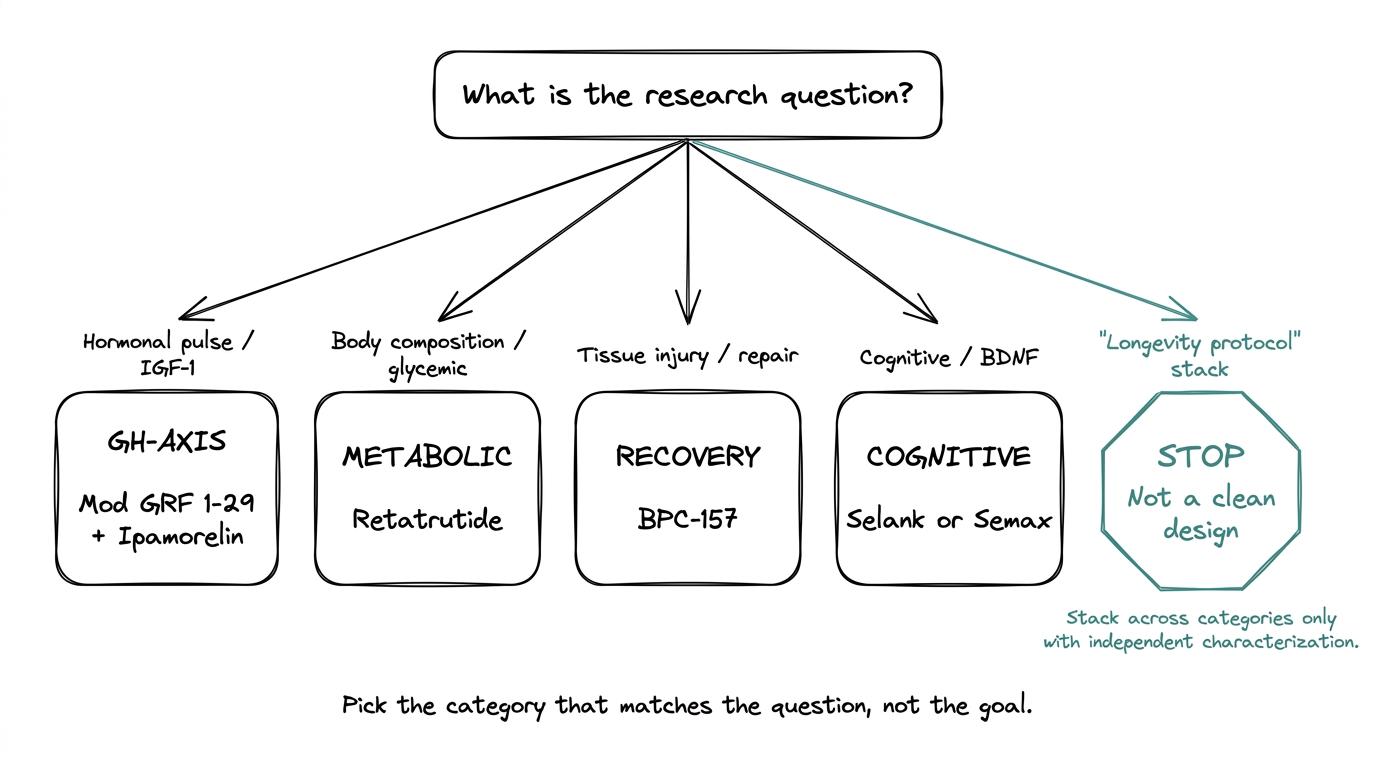
Pick GH-axis
When the research question is hormonal — pulse architecture, IGF-1 dynamics, body composition through GH-mediated effects, or sleep-GH coupling.
Pick metabolic
When the research question is body-composition through energy balance, glycemic control, or hepatic fat oxidation. Note that metabolic peptide work overlaps with GH-axis work in body-composition outcomes — the mechanism difference matters for clean experimental design.
Pick recovery
When the research model involves tissue injury, gastrointestinal repair, or angiogenesis-dependent healing. The longevity-framing here is indirect: recovery capacity as a resilience proxy rather than a direct aging intervention.
Pick cognitive
When the model targets BDNF pathway modulation, acute cognitive performance, or neuroprotection in stress and ischemia paradigms.
Multi-category stacking
Stack across categories only when the experimental design can distinguish individual contributions. A GH-axis stack plus a recovery compound is a defensible research design when each variable is independently characterized. A four-category stack as a “longevity protocol” is not a clean research design and is not a framing this site supports.
What the longevity literature actually shows
The honest read on the longevity-research peptide literature:
- ●Most published work is preclinical (rodent and cell-culture models).
- ●Lifespan-extension data from peptide compounds is overwhelmingly limited to short-lived model organisms (worms, flies, some rodent studies).
- ●Clinical longevity outcomes data — humans living measurably longer because of peptide protocols — does not exist in any published controlled form.
- ●Healthspan-related outcomes (functional measures, biomarkers, body composition in middle-aged adults) have stronger but still preliminary clinical signal for the GH-axis and metabolic categories specifically.
That is the limit of the evidence. Anyone claiming peptide protocols extend human lifespan is going beyond what the published literature currently supports.
Quality signals across all four categories
For sourcing any of the compounds covered above, the quality requirements are the same.
- ●HPLC purity above 98% with a batch-specific Certificate of Analysis per vial.
- ●Mass spectrometry identity confirmation matching the expected molecular weight.
- ●Sequence verification on the COA where applicable.
- ●Cold-chain discipline in transit and storage.
The peptide Certificate of Analysis guide walks through what a real COA contains and the four red flags that signal repackaged or mislabeled material. The same checks apply across categories.
Where to go from here
For deeper compound-level coverage:
- ●The CJC-1295 + Ipamorelin explainer covers the GH-axis stack mechanism.
- ●The retatrutide explainer covers the metabolic / triple-agonist frontier.
- ●The BPC-157 vs TB-500 comparison covers the recovery-category mechanism distinctions.
- ●The retatrutide vs Ozempic comparison covers the metabolic-category benchmark difference.
For vendor evaluation, the best peptide vendors 2026 framework covers the five-criteria evaluation that applies across the line.
Quick reference
- ●"Peptides for longevity" is a search category, not a pharmacological category.
- ●Four research-peptide categories intersect the longevity conversation: GH-axis, metabolic, recovery, cognitive.
- ●GH-axis (Mod GRF 1-29 + Ipamorelin) is the load-bearing category in research-peptide longevity work.
- ●Metabolic (retatrutide), recovery (BPC-157), and cognitive (Selank, Semax) sit alongside as distinct categories with distinct mechanisms.
- ●The line excludes compounds with thinner research and "anti-aging" marketing framing (Epitalon, MOTS-c, GHK-Cu, etc.). The category map is transparent about what is and is not in scope.
- ●No published controlled clinical lifespan data exists for peptide compounds. Healthspan-related signal is preliminary and category-specific.
Frequently asked questions
Do peptides extend human lifespan?
No published controlled clinical data shows peptide protocols extend human lifespan. Lifespan-extension data is limited to short-lived model organisms. Healthspan-related outcomes have stronger but still preliminary clinical signal for GH-axis and metabolic categories.
What is the best peptide for anti-aging?
There is no single "anti-aging peptide." Different peptides address different aging-related systems: GH-axis compounds (Mod GRF 1-29 + Ipamorelin) for hormonal decline, metabolic peptides (retatrutide) for metabolic dysregulation, recovery peptides (BPC-157) for tissue repair, and cognitive peptides (Selank, Semax) for neurotransmitter modulation.
What compounds does The Peptide Lab carry for longevity research?
Six compounds across four categories: Mod GRF 1-29 and Ipamorelin (GH-axis), Retatrutide (metabolic), BPC-157 (recovery), and Selank and Semax (cognitive). Compounds like Epitalon, MOTS-c, and GHK-Cu are deliberately excluded.
Why does The Peptide Lab not carry Epitalon or GHK-Cu?
Compounds with thinner published research, marketing-driven "anti-aging" framing, or unclear regulatory positioning sit outside the line. The category map is transparent about what is and is not in scope.
Can I stack peptides from different longevity categories?
Only when the experimental design can distinguish individual contributions. A GH-axis stack plus a recovery compound is defensible when each variable is independently characterized. A four-category "longevity protocol" stack is not a clean research design.
What is the most-researched longevity peptide category?
The GH-axis category, anchored by the Mod GRF 1-29 + Ipamorelin stack, has the deepest research base. It addresses age-related GH pulse-amplitude decline, body composition, sleep architecture, and IGF-1 dynamics.
Next step
Explore the research-peptide line
Six compounds across four longevity-adjacent categories, each with batch-specific COAs and transparent quality documentation.